ACLS Review Questions
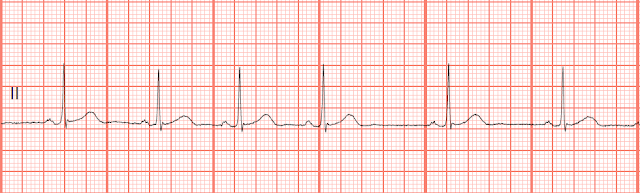
4. You are dispatched to the home of a man who “passed out” during a family picnic. When you arrive at the scene 4 minutes later you find the patient is unresponsive, pulseless and apneic. Bystander CPR has not been initiated. As you begin CPR and your partner places the monitor pads on the patient, the following rhythm is observed:

What is the most appropriate intervention at this time?
A. Defibrillate the patient at 120-200 J
B. Continue CPR as your partner inserts an endotracheal tube
C. Start an IV and administer epinephrine 1mg IV
D. Administer Amiodarone 300mg IV
Answer A. Defibrillate the patient at 120-200 J
Early defibrillation is a link in the AHA chain of survival and is the treatment of choice for pulseless ventricular fibrillation. CPR provides oxygen, substrate, and blood flow to the myocardium but has little effect on the fibrillating heart. Immediate defibrillation works by depolarizing the myocardium so that SA node will begin providing the pacing stimulus for the heart. The initial joule setting will depend upon the manufactures recommendations for the brand of monitor that is being used, but usually this falls within the 120-200 J range. If it is not known, then the AHA suggests that the initial joule setting be 200 J for a biphasic monitor and 360 J for a monophasic monitor. Answer B is not an appropriate intervention at this time. Intubation at the scene may not be necessary if positive pressure ventilations are adequate. Answer C: Although epinephrine is one of the first vasoconstrictors to be administered during a VF cardiac arrest, immediate defibrillation is the first treatment option. If the VF remains refractory to the initial defibrillation attempts, then the next intervention would be to administer either epinephrine or vasopressin. Answer D: Amiodarone is the first antiarrhythmic agent to be given in a pulseless VF/VT arrest but it is given after the vasoconstrictors and repeated defibrillation attempts.
Reviewed 3/1/16
Reviewed 3/1/16


Comments
Post a Comment