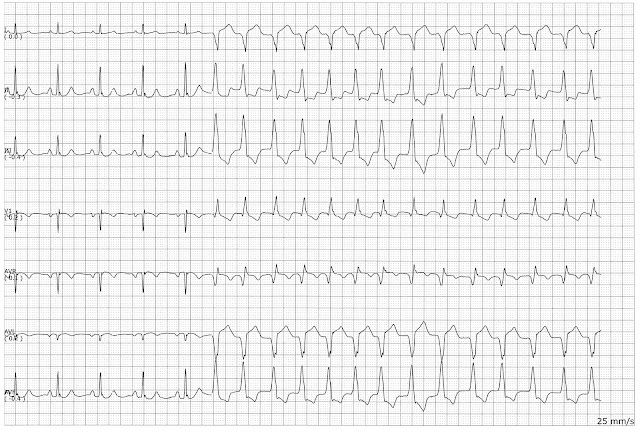
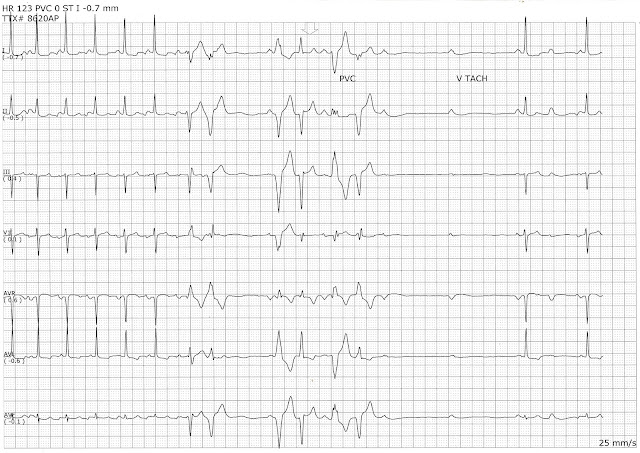
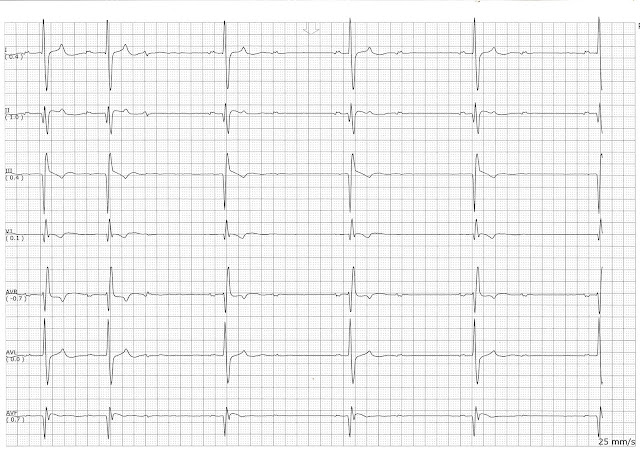
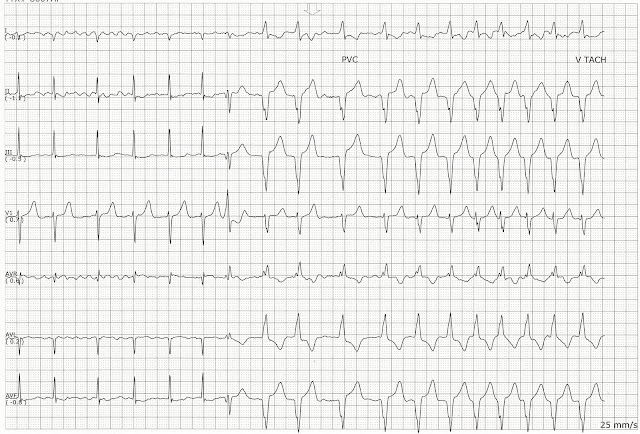
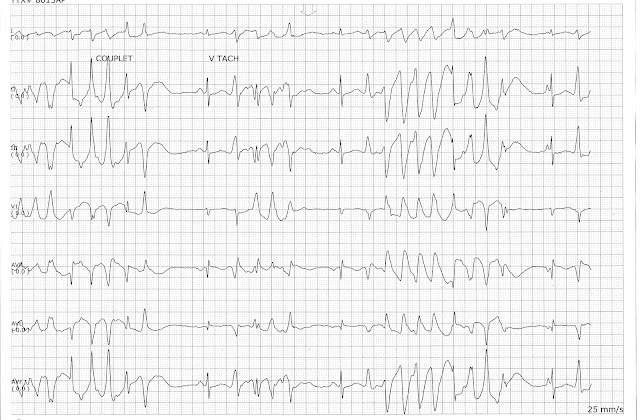
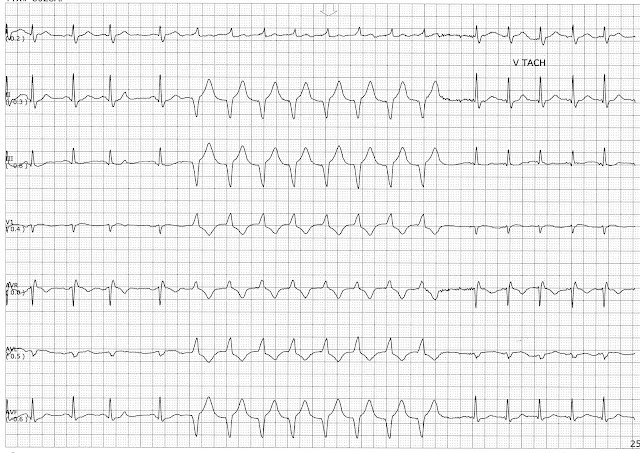
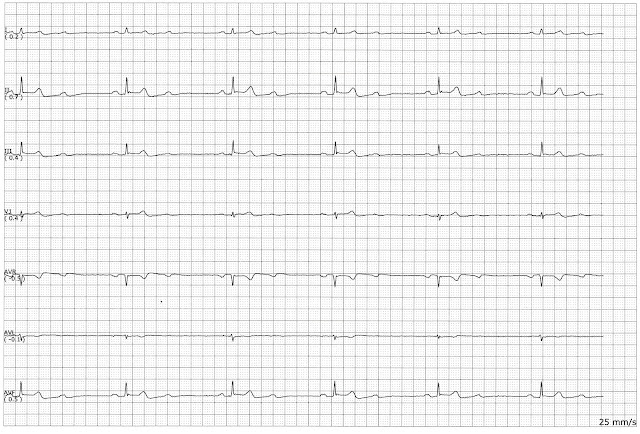
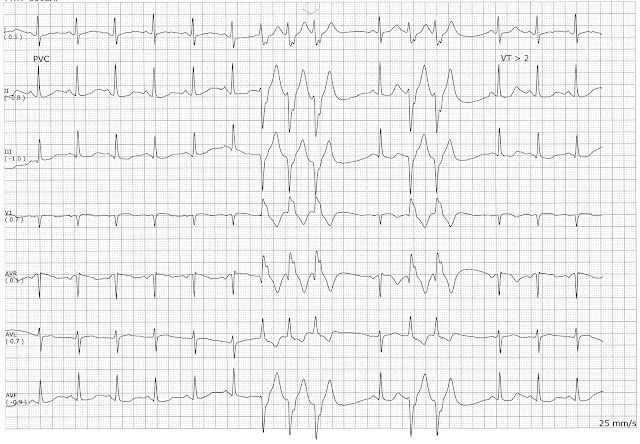
These three rhythms strips belong to the same patient. If you examine the morphology of the early beats in the first two strips you can seen the same morphological changes in the T wave when a nonconducted PAC occurs. In the very last strip, those same characteristics are seen in a bigeminal pattern. In this strip, the patient is showing what appears to be aberrantly conducted PACs in a quadrigeminal pattern. The change in the height of the T wave before each ectopic beat leads me to believe that they are atrial in origin. I have circled the ectopic P waves for comparison in the next strips. In this second strip. The early beat of complex 4 shows the same kind of P wave. Then another nonconducted P wave is seen after complex 5. If you look at the morphology of these P waves in aVL the look the same. The same pattern is seen in complexes 9 and the nonconducted beat after complex 10 Keeping in mind the morphological similar...