Pediatric cardiac arrest: PEA
1250: A 10 year old
boy is brought to the emergency room by EMS after he struck a tree with his three-wheeler. On the scene he was conscious, alert and oriented but in route he began to
have increasing shortness of breath and was becoming more lethargic. The EMTs initiated positive pressure ventilations
in route to the hospital. He is on a
spinal board with a C collar in place.
When he is transferred from the EMS stretcher to the hospital stretcher
is found to be unresponsive and he no longer has spontaneous respirations.
1252: No pulse is detected. A pediatric code
is called and CPR is initiated. He is
placed on the monitor and this is his initial rhythm.
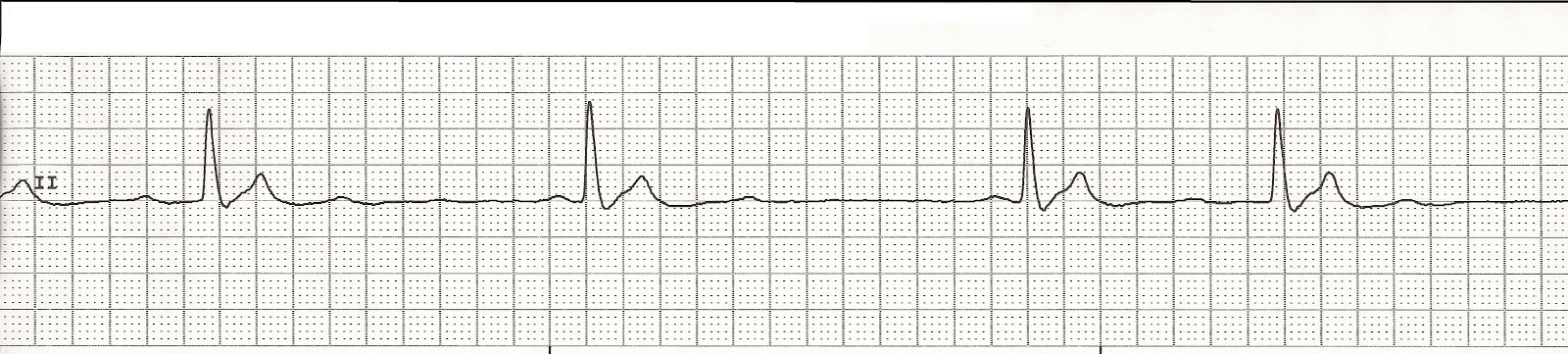 |
| PEA rhythm |
1255: CPR is continued. A #20 IV is started in his right antecubtial fossa. Epinephrine 1mg IV is given and and a fluid bolus of 20ml/kg is also
started. Because there is difficulty
with providing positive pressure ventilations, the patient is intubated with a
6.5 cuffed ET tube.
1255: A review of his
medical history is as follows
Symptoms: no symptoms
prior to accident. A healthy 10 year old
male child
Allergies: allergic
to Augmentin which causes a systemic rash
Medications: a daily chidlren's multivitamin
Past medical history: a tonsillectomy 2 years ago, seasonal
allergies.
Last meal eaten: last
oral intake estimated to be at 0800 that morning
Events: His friends
stated that he was driving racing his friend on his three-wheeler and lost control and hit a tree at
high speed. He was wearing a helmet at
the time.
1256: Physical exam is as follows
Neuro: unresponsive, Glasgow
score of 8
EENT: pupils
nonreactive, no facial or head trauma
Neck: tracheal deviation to the left
Lungs: Intubated with
6.5 ET tube. Positive end tidal CO2
indicators. Difficult to ventilate with
positive pressure ventilations. Auscultation
of chest reveals good breath sounds on the right but decreased breath sounds on the left and no gurgling over the
epigastrium. There is asymmetrical chest
rise. There is bruising and swelling on the left chest wall.
Abdomen: bruising on
the left side of the upper abdomen. Mild
stomach distension.
Gentialia: No bleeding from the urinary meatus. A urinary catheter is being placed.
Extremities: Abrasions
to left shoulder and arm. Left shoulder
is posteriorly displaced. Lower extremities unremarkable
Labs: CBC, comprehensive
metabolic panel, type and cross match
Radiology: CXR, Left
shoulder, clavicle, left arm. CT head, neck,
abdomen, and pelvis.
1259: CPR is in
progress and epinephrine 0.01mg/kg is repeated.
A 2nd fluid bolus is initiated.
 |
| CPR rhythm |
13:01: Because of the tracheal deviation and asymmetrical
chest rise, a needle decompression is performed which causes an immediate
improvement in the ease of ventilations and the patient also begins to have
symmetrical chest rise.
1305: CPR continues. EpInephrine 0.01mg/kg is given.
 |
| CPR rhythm |
1308: A rhythm check reveals a change in the
patient’s rhythm
 |
| Sinus bradycardia without a pulse |
1309: The patient
remains pulseless and apneic. CPR is
continued.
 |
| CPR rhythm |
1310: Another dose of
epinephrine is given and another fluid bolus of 20mg/kg is ordered.
1314: Another rhythm check reveals the following
rhythm.
 |
| Sinus tachycardia |
1315: At this time a
carotid and brachial pulse are detected.
Vital signs: 97.2-120-20. BP 84/54.
Oxygen saturation 93%. The
patient is beginning to have spontaneous, shallow respirations. Positive pressure ventilations are continued
and another fluid bolus of 20ml/kg is given.
Portable X-ray studies are completed at the bedside and preparations are
being made to transport the patient to radiology for the CT studies.
Final diagnosis:
CT head and neck: negative
Left shoulder X-ray:
displaced fracture of the left clavicle and proximal humerus.
Chest x ray:
Pneumothorax and left 9-12 rib fractures.
CT abdomen: a splenic
hematoma with contrast extravasation and some contrast pooling on delayed images with free
fluid in the abdomen.
CBC: Hgb 9.2
and HCT 10.3
Chemistries:
WNL
Type and Cross match: O positive blood.



Comments
Post a Comment